

Vulvar allodynia is a recognized complication of the transvaginal mesh. It interferes with physical, sexual, and psychosocial function “
 (Vaginal Mesh Implant Complication News) Women who have had vaginal mesh implantation surgery often wonder whether wearing tight pants will cause them pain. Vulvar allodynia is a “super sensitivity of the vulva” which causes normal sensations such as a gentle touch or minimal friction from tight fitting clothes to be exquisitely painful. This condition could be generalized, affecting the entire vulva or localized affecting a specific side of the vulva or structure of the vulva such as the clitoris. This pain can cause painful sexual intercourse, it interferes with sitting, it interferes with mobility, and makes wearing tight fitting pants painful because the normal friction of the clothes will cause significant pain. Experts in the field state that vulvar allodynia should be thought of by doctors as Complex Regional Pain Syndrome (CRPS) which was historically called Reflex Sympathetic Dystrophy (RSD). Symptoms form CRPS vary but most commonly consist of stinging and burning.
(Vaginal Mesh Implant Complication News) Women who have had vaginal mesh implantation surgery often wonder whether wearing tight pants will cause them pain. Vulvar allodynia is a “super sensitivity of the vulva” which causes normal sensations such as a gentle touch or minimal friction from tight fitting clothes to be exquisitely painful. This condition could be generalized, affecting the entire vulva or localized affecting a specific side of the vulva or structure of the vulva such as the clitoris. This pain can cause painful sexual intercourse, it interferes with sitting, it interferes with mobility, and makes wearing tight fitting pants painful because the normal friction of the clothes will cause significant pain. Experts in the field state that vulvar allodynia should be thought of by doctors as Complex Regional Pain Syndrome (CRPS) which was historically called Reflex Sympathetic Dystrophy (RSD). Symptoms form CRPS vary but most commonly consist of stinging and burning.
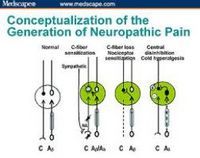
Reflex Sympathetic Dystrophy is a horrific pain syndrome caused from either soft tissue injury or peripheral nerve injury. Recently the medical community has attempted to change the name of RSD into CRPS Type 1 or CRPS Type 2. CRPS Type 1 occurs in the absence of nerve injury and CRPS Type 2 occurs where there is an identified nerve lesions. Although the mechanism of both CRPS Type 1 and CRPS Type 2 have not been fully determined it is believed to be the result of both central nervous system changes that result from peripheral nervous tissue inflammation and peripheral nervous system changes that result from inflammation.
How does a vaginal mesh implant cause CRPS Type 1 and CRPS Type 2?
CRPS Type 1 occurs in the absence of identified nerve injury and can be the result of myofascial hypertonicity or primary myofascial pain (commonly referred in the literature as pelvic pain tension myalgia) It is recognized that the transvaginal mesh causes both primary myofascial pain by direct irritation or inflammation of the muscles of the pelvic floor. The surgery itself may cause primary myofascial pain which can then cause vulvar allodynia.
CRPS Type 2 occurs in the presence of identified nerve lesions. It has been well established that the transvaginal mesh and the transvaginal mesh procedure can cause both obturator and pudendal neuralgia, known vaginal mesh complications. It also has been well established that the terminal branches of the pudendal nerve which include the clitoril, perineal, and the inferior rectal branch can be damaged by the mesh or by the procedure. Any of these identifiable nerve injuries can cause vulvar allodynia via CRPS Type 2.
Treatment of vulvar allodynia is based on the concept of functional restoration. Treatment is aimed at decreasing muscle spasm, restoring range of motion, improving the strength of the pelvic muscles. This is obtained by medications both oral and local acting and pelvic physical therapy which will consist of intravaginal and intrarectal message, message to the pelvic girdle muscles, stretching and strengthening. Biofeedback is a useful modality in these patients because it allows them to visualize their own muscle tension via monitors placed onto muscles of the pelvic girdle and this provides a means for the patients to learn how to control their own pelvic tension. In patients who fail to progress in physical therapy injections of either Botox or local anesthetics may be attempted with hopes that these interventions will allow the patient to progress with ongoing therapy. If the pain does not improve, selected patients may require the entire mesh to be removed, and others may require injections via CT guided pudendal nerve block of the main trunk or the peripheral branches. Pudendal nerve decompression of either the main branch and the terminal branches may also be necessary if these are determined to be the pain generators.
Chronic vulvar allodynia may persist despite these interventions and patients will require life long medication management, psychological counseling, and physical therapy to manage their pain and maintain their function.
For more information on vaginal mesh implant complications please visit www.TVM123.com today.
Social Media Tags: painful sexual intercourse, reflex sympathetic dystrophy, myofascial pain, nervous tissue, peripheral nerve injury, regional pain syndrome, tension myalgia, allodynia,




