

Implantable stimulators to the spinal cord have been historically used for chronic pain from spinal disorders and RSD. Now it is used for chronic pelvic pain. “
 Medical Perspective:
Medical Perspective:
Historically, electric therapy has been recognized as a potential treatment for pain since the Egyptians noted that the electrical discharges of the Nile catfish helped painful conditions including neuralgias. The first published use of electric therapy was in ancient Rome where torpedo fish were used to shock gout pain. Despite its recognized benefit, electric therapy remained out of the mainstream of medical care and had been referred to as ‘quackery’. This changed in the 1965 after Melzak and Wall presented the “Gate Control Theory” of pain transmission by stimulating the larger fiber nerve cells, it would block or close the gate to the small fiber nerve cells that transmit pain. The first clinical use of implanted nerve stimulation to the spinal cord was in 1967. There are many possible mechanisms of pain transmission and there is little consensus whether electric therapy decreases pain. Regardless of which mechanism electric therapy affects, it has been a proven treatment for RSD and failed back surgery syndrome for the past forty years and is more effective on painful conditions from the peripheral nervous system as opposed to the central nervous system (spinal cord and brain). Originally, the electrical current was directed onto the ‘dorsal root’ of the spinal cord, which contains the sensory fibers. More recently, pain physicians have noted significant pain control by direct placement of the electrical current on a peripheral nerve that is responsible for a painful condition that is confined to its nerve distribution.
Who is a candidate for spinal stimulation or peripheral nerve stimulation?
Chronic intractable pain causes a significant economic burden on the patient and society. The functional, psychosocial, and medical damages of the patient and family are immeasurable. Spinal cord stimulation and peripheral nerve stimulation should be considered in any patient who suffers from continued intractable pain who have failed all conservative efforts and surgical efforts to improve their pain. It is my opinion as a physician managing pain for many years, that any patient who has pain that is related to neural compression that can be surgically decompressed should not be considered a candidate for peripheral nerve stimulation or spinal cord stimulation since there is a potential reversible problem.
What is the role of spinal stimulation or peripheral nerve stimulation in a pelvic pain patient?
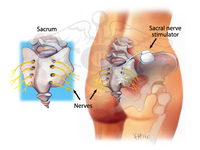
The role of spinal stimulation and peripheral nerve stimulation is evolving as the clinical experience with these modalities increase and are published by the leading centers in the world. ?A leading expert in Switzerland, Dr. Marc Possover, published a paper concerning his experience with the use of spinal stimulation. He reserves if for the patients who fail medical treatment including surgical decompression of the pudendal nerve or if the patient continues to have pain despite medical treatment and on surgical evaluation, there is no evidence of nerve compression. In a small sample of patients who had pudendal neuralgia because of compression at the sacrotuberous ligament that failed to improve with decompression, all had improvement in their pain with spinal stimulation with the electrode at the S2, S3, and S4/5 nerve roots. The author noted that the most difficult group of patients in his series to manage were the patients with nerve damage from mesh procedures and the non-mesh related complications for the treatment of prolapse. In these patients there where eight who continued to have significant pain that was pudendal-like despite decompression of the nerves with five of the eight having improvement with spinal stimulation. The author states that the study was limited by its small sample size but does offer what he describes as the final hope for improvement in these patients.
Another study in the United States suggests that electrode placement at the pudendal nerve may benefit patients who do not improve with spinal stimulation. This study involved patients with a variety of problems including frequency, urgency, and pelvic pain. The role of peripheral stimulation to the pudendal nerve appears to be viable therapeutic option in the future.
What does this means for a transvaginal mesh implant patient?
Patients with persistent intractable pain following pudendal decompression (understanding that some patients are improving with another attempt at decompression) and patients with persistent pain despite all other therapeutic interventions who are determined to not have a compressive lesion to the pudendal nerves and its branches should be considered for either spinal stimulation at the sacral nerve roots or peripheral stimulation at the pudendal nerve roots. A trial as an outpatient will be carried out with an external stimulator with a wire placed to the nerve or nerve roots. If pain relief is significant the patient will be a candidate for implantation.
Life Care Planning Perspective:
A life care planner must consider the life-long treatments required in the management of pain related to the side effects of a transvaginal mesh procedure. The life care planner must understand the studies that indicate repeat decompression may be required for a failed decompression or for pain that returns. The life care planner must understand that patients with continued pain must be referred to a center of excellence that manages both mesh removal, nerve decompression, and all other treatment options for post-transvaginal mesh related pain. If at the center of excellence the patient is determined to have no further compressive lesion on the nerves in the pelvis, only then can sacral stimulation or peripheral stimulation be attempted. A life care planner must be educated on the aspects of post-mesh related pain, educate the public, and provide a plan that includes these therapeutic options if determined to be medically necessary and appropriate by the patient’s treating physician. Any patient who receives a stimulator must have a life care plan that takes into account the cost associated including replacement, medical follow ups, and all future care related to the device.
Learn more about the unique advantages of Life Care Solutions Group by visiting their Vaginal Mesh Website.
Social Media Tags: spinal cord stimulation, gate control theory of pain, chronic intractable pain, peripheral nerve, pudendal nerve, pudendal neuralgia, transvaginal mesh




